|
Overview
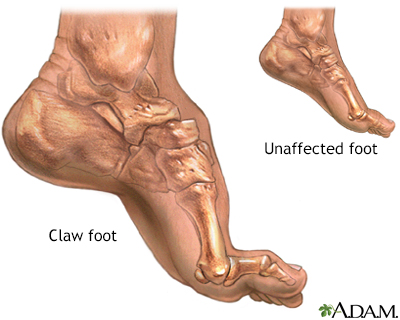 Basically, fallen arches refers to a flattening of the feet that takes place in adulthood. Although there may be other causes, this flattening usually occurs when the tendon (posterior tibial tendon) and ligaments that hold the arch in place gradually stretch. As we get older and our cumulative use of these tendons and ligaments increases, they lose their ability to maintain that nice arch shape, and may even begin to tear. This stretching or tearing may also be the result of an injury, obesity, or a genetic predisposition for flat feet. Causes Most cases of flatfeet are simply the result of normal development. When that is not the case, the condition can be caused by a number of factors, including the following, Age, disease, injury, obesity or being overweight, physical abnormality, pregnancy. Flattened arches in adults may result from the stresses of aging, weight gain, and the temporary increase in elastin (protein in connective tissue) due to pregnancy. In some cases, flatfeet are caused by a physical abnormality, such as tarsal coalition (two or more bones in the foot that have grown together) or accessory navicular (an extra bone along the side of the foot). The effects of diseases such as diabetes and rheumatoid arthritis can lead to flatfeet. An injury (e.g., bone fracture, dislocation, sprain or tear in any of the tendons and ligaments in the foot and leg) also can cause flatfeet. Symptoms Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle. Diagnosis Your doctor will ask about your symptoms and medical history. A physical and foot exam will be done. Flat feet can be diagnosed by appearance. To determine if the foot is rigid, you may be asked to do some simple tasks. fallen arches exercises Non Surgical Treatment Treatment of flat feet may be appropriate if there is associated foot or lower leg pain, or if the condition affects the knees or the lower back. Treatment may include using Orthoses such as an arch support, foot gymnastics or other exercises as recommended by a podiatrist/orthotist or physical therapist. In cases of severe flat feet, orthoses should be used through a gradual process to lessen discomfort. Over several weeks, slightly more material is added to the orthosis to raise the arch. These small changes allow the foot structure to adjust gradually, as well as giving the patient time to acclimatise to the sensation of wearing orthoses. Once prescribed, orthoses are generally worn for the rest of the patient's life. In some cases, surgery can provide lasting relief, and even create an arch where none existed before; it should be considered a last resort, as it is usually very time consuming and costly. Surgical Treatment  Fallen arches may occur with deformities of the foot bones. Tarsal coalition is a congenital condition in which the bones of the foot do not separate from one another during development in the womb. A child with tarsal coalition exhibits a rigid flat foot, which can be painful, notes the patient information website eOrthopod. Surgery may prove necessary to separate the bones. Other foot and ankle conditions that cause fallen arches may also require surgery if noninvasive treatments fail to alleviate pain and restore normal function. After Care Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low. Overview
 When walking, your heels repeatedly hit the ground with considerable force. They have to be able to absorb the impact and provide a firm support for the weight of the body. When pain develops in the heel, it can be very disabling, making every step a problem, affecting your posture. There are various types of heel pain. Some of the most common are: heel spurs (plantar fasciitis); heel bursitis and heel bumps. Causes Heel pain has a number of causes that are typically associated with overuse of the heel bone. You can strain your heel by pounding your feet on hard surfaces, being overweight, or wearing shoes that do not fit properly. These strains can irritate the heel?s bones, muscles, or tendons. Other common causes of heel pain include the following. Heel Spurs. Heel spurs develop when the lining that covers the heel is continuously stretched. When this occurs, pieces of the lining may break off. Heel spurs typically develop in athletes who frequently run or jog. They are also common in people who are obese. Plantar Fasciitis. Plantar fasciitis develops when the tissue connecting the heel to the ball of the foot becomes inflamed. Plantar fasciitis also occurs in athletes who frequently run or jog. It can also result from wearing shoes that do not fit properly. Excessive Pronation. Excessive pronation occurs when the ligaments and tendons at the back of the heel are stretched too much. This condition can occur when injuries to the back, hips, or knees change the way you walk. Achilles Tendinitis. Achilles tendinitis can occur when the Achilles tendon, which runs along the back of the heel, becomes inflamed. This condition is common in people with active lifestyles who frequently run and jog, professional athletes and dancers. Symptoms Usually when a patient comes in they?ll explain that they have severe pain in the heel. It?s usually worse during the first step in the morning when they get out of bed. Many people say if they walk for a period of time, it gets a little bit better. But if they sit down and get back up, the pain will come back and it?s one of those intermittent come and go types of pain. Heel pain patients will say it feels like a toothache in the heel area or even into the arch area. A lot of times it will get better with rest and then it will just come right back. So it?s one of those nuisance type things that just never goes away. The following are common signs of heel pain and plantar fasciitis. Pain that is worse first thing in the morning. Pain that develops after heavy activity or exercise. Pain that occurs when standing up after sitting for a long period of time. Severe, toothache type of pain in the bottom of the heel. Diagnosis After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests. Non Surgical Treatment Treating plantar fasciitis in the early stages usually allows for a quicker recovery. Left untreated, this condition can progress to the point where there is pain with each and every step. This typically means a return to a pain free day will take much longer. Initial treatments are aimed at reducing stress on the fascia so it can begin to heal. Also, treatment to reduce the associated inflammation is started. These treatments often include: ice therapy, anti-inflammatory medications, stretching exercises, wearing shoes with appropriate support, taping of the foot and the use of a night splint. If these interventions do not lead to a full resolution, custom shoe inserts, cortisone injections and additional treatment by a physical therapist are often utilized. For patients that fail to respond to all of these efforts, surgical release of the plantar fascia can be a very effective course of action. The good news is this: 95% of the time plantar fasciitis can be fully resolved without the need for surgery. High energy shock wave therapy, sometimes referred to as orthotripsy, is a relatively new treatment that has been shown to be effective 70% of the time in patients that continue to have pain despite extensive non-surgical treatment. Surgical Treatment If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team. heel spur shoes Prevention  Preventing heel pain is crucial to avoid pain that can easily interrupt a busy or active lifestyle. Athletes can prevent damage by stretching the foot and calf both before and after an exercise routine. The plantar fascia ligament can be stretched by using a tennis ball or water bottle and rolling it across the bottom of the foot. With regular stretching, the stretching and flexibility of tissue through the foot can be significantly improved, helping to prevent damage and injury. Athletes should also ease into new or more difficult routines, allowing the plantar fascia and other tissue to become accustomed to the added stress and difficulty. Running up hills is also common among athletes in their routines. However, this activity should be reduced since it places an increased amount of stress on the plantar fascia and increases the risk of plantar fasciitis. Maintaining a healthy weight is also an essential heel pain prevention technique. Obesity brings additional weight and stress on the heel of the foot, causing damage and pain in the heel as well as in other areas of the foot. Overview
Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician.  Causes There are many causes of leg length discrepancy. Some include, A broken leg bone may lead to a leg length discrepancy if it heals in a shortened position. This is more likely if the bone was broken in many pieces. It also is more likely if skin and muscle tissue around the bone were severely injured and exposed, as in an open fracture. Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. A break in a child's bone through the growth center near the end of the bone may cause slower growth, resulting in a shorter leg. Bone infections that occur in children while they are growing may cause a significant leg length discrepancy. This is especially true if the infection happens in infancy. Inflammation of joints during growth may cause unequal leg length. One example is juvenile arthritis. Bone diseases may cause leg length discrepancy, as well. Examples are, Neurofibromatosis, Multiple hereditary exostoses, Ollier disease. Other causes include inflammation (arthritis) and neurologic conditions. Sometimes the cause of leg length discrepancy is unknown, particularly in cases involving underdevelopment of the inner or outer side of the leg, or partial overgrowth of one side of the body. These conditions are usually present at birth, but the leg length difference may be too small to be detected. As the child grows, the leg length discrepancy increases and becomes more noticeable. In underdevelopment, one of the two bones between the knee and the ankle is abnormally short. There also may be related foot or knee problems. Hemihypertrophy (one side too big) or hemiatrophy (one side too small) are rare leg length discrepancy conditions. In these conditions, the arm and leg on one side of the body are either longer or shorter than the arm and leg on the other side of the body. There may also be a difference between the two sides of the face. Sometimes no cause can be found. This is known as an "idiopathic" difference. Symptoms As patients develop LLD, they will naturally and even unknowingly attempt to compensate for the difference between their two legs by either bending the longer leg excessively or standing on the toes of the short leg. When walking, they are forced to step down on one side and thrust upwards on the other side, which leads to a gait pattern with an abnormal up and down motion. For many patients, especially adolescents, the appearance of their gait may be more personally troublesome than any symptoms that arise or any true functional deficiency. Over time, standing on one's toes can create a contracture at the ankle, in which the calf muscle becomes abnormally contracted, a condition that can help an LLD patient with walking, but may later require surgical repair. If substantial enough, LLD left untreated can contribute to other serious orthopaedic problems, such as degenerative arthritis, scoliosis, or lower back pain. However, with proper treatment, children with leg length discrepancy generally do quite well, without lingering functional or cosmetic deficiencies. Diagnosis Leg length discrepancy may be diagnosed during infancy or later in childhood, depending on the cause. Conditions such as hemihypertrophy or hemiatrophy are often diagnosed following standard newborn or infant examinations by a pediatrician, or anatomical asymmetries may be noticed by a child's parents. For young children with hemihypertophy as the cause of their LLD, it is important that they receive an abdominal ultrasound of the kidneys to insure that Wilm's tumor, which can lead to hypertrophy in the leg on the same side, is not present. In older children, LLD is frequently first suspected due to the emergence of a progressive limp, warranting a referral to a pediatric orthopaedic surgeon. The standard workup for LLD is a thorough physical examination, including a series of measurements of the different portions of the lower extremities with the child in various positions, such as sitting and standing. The orthopaedic surgeon will observe the child while walking and performing other simple movements or tasks, such as stepping onto a block. In addition, a number of x-rays of the legs will be taken, so as to make a definitive diagnosis and to assist with identification of the possible etiology (cause) of LLD. Orthopaedic surgeons will compare x-rays of the two legs to the child's age, so as to assess his/her skeletal age and to obtain a baseline for the possibility of excessive growth rate as a cause. A growth chart, which compares leg length to skeletal age, is a simple but essential tool used over time to track the progress of the condition, both before and after treatment. Occasionally, a CT scan or MRI is required to further investigate suspected causes or to get more sophisticated radiological pictures of bone or soft tissue. Non Surgical Treatment The treatment of LLD depends primarily on the diagnosed cause, the age of the patient, and the severity of the discrepancy. Non-operative treatment is usually the first step in management and, in many cases, LLD is mild or is predicted to lessen in the future, based on growth rate estimates in the two legs. In such cases, no treatment may be necessary or can be delayed until a later stage of physical maturity that allows for clearer prognostic approximation. For LLD of 2cm to 2.5cm, treatment may be as simple as insertion of a heel lift or other shoe insert that evens out leg lengths, so to speak. For more severe cases, heel lifts can affect patient comfort when walking, decrease ankle stability, and greatly increase the risk of sprains. For infants with congenital shortening of the limb, a prosthetic ? often a custom-fit splint made of polypropylene ? may be successful in treating more severe LLD without surgery. In many instances, however, a surgical operation is the best treatment for LLD.  shoe lifts for uneven legs Surgical Treatment Shortening techniques can be used after skeletal maturity to achieve leg length equality. Shortening can be done in the proximal femur using a blade plate or hip screw, in the mid-diaphysis of the femur using a closed intramedullary (IM) technique, or in the tibia. Shortening is an accurate technique and involves a much shorter convalescence than lengthening techniques. Quadriceps weakness may occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done. If the femoral shortening is done proximally, no significant weakness should result. Tibial shortening can be done, but there may be a residual bulkiness to the leg, and risks of nonunion and compartment syndrome are higher. If a tibial shortening is done, shortening over an IM nail and prophylactic compartment release are recommended. We limit the use of shortenings to 4 to 5 cm leg length inequality in patients who are skeletally mature. Overview
 Morton's neuroma is an enlarged nerve that usually occurs in the third interspace, which is between the third and fourth toes. To understand Morton's neuroma further, it may be helpful to look at the anatomy of the foot. Problems often develop in the third interspace because part of the lateral plantar nerve combines with part of the medial plantar nerve here. When the two nerves combine, they are typically larger in diameter than those going to the other toes. Also, the nerve lies in subcutaneous tissue, just above the fat pad of the foot, close to an artery and vein. Above the nerve is a structure called the deep transverse metatarsal ligament. This ligament is very strong, holds the metatarsal bones together, and creates the ceiling of the nerve compartment. With each step, the ground pushes up on the enlarged nerve and the deep transverse metatarsal ligament pushes down. This causes compression in a confined space. Morton's neuroma is an enlarged nerve that usually occurs in the third interspace, which is between the third and fourth toes. To understand Morton's neuroma further, it may be helpful to look at the anatomy of the foot. Problems often develop in the third interspace because part of the lateral plantar nerve combines with part of the medial plantar nerve here. When the two nerves combine, they are typically larger in diameter than those going to the other toes. Also, the nerve lies in subcutaneous tissue, just above the fat pad of the foot, close to an artery and vein. Above the nerve is a structure called the deep transverse metatarsal ligament. This ligament is very strong, holds the metatarsal bones together, and creates the ceiling of the nerve compartment. With each step, the ground pushes up on the enlarged nerve and the deep transverse metatarsal ligament pushes down. This causes compression in a confined space.Causes There are many reasons to develop a neuroma. Improper shoe gear is probably the most likely cause. Repetitive activity and excessive pressure on the ball of the foot are common. Heredity and genetic factors may also be involved. In many cases the structure of the foot may predispose the condition. Associated conditions that may cause neuroma include: bunion, hammer toes, ligament laxity, and/or a tight calf muscle. Some patients may have thinning of the fat pad on the ball of the foot, which may result in increased pressure of the nerves. Tight pointy shoes (and high heels) without padding may induce pain in the ball of the foot. Neuroma may occur suddenly, or develop over time. Symptoms Morton's neuroma can cause a very painful burning or sharp pain in your foot that feels worse when you walk. It may feel like a small lump inside the ball of your foot. It is usually between the third and fourth toes, but it can also be between other toes. Diagnosis To diagnose Morton's neuroma the podiatrist commonly palpates the area to elicit pain, squeezing the toes from the side. Next he or she may try to feel the neuroma by pressing a thumb into the third interspace. The podiatrist then tries to elicit Mulder's sign, by palpating the affected interspace with one hand and squeezing the entire foot at the same time with the other hand. In many cases of Morton's neuroma, this causes an audible click, known as Mulder's sign. An x-ray should be taken to ensure that there is not a fracture. X-rays also can be used to examine the joints and bone density, ruling out arthritis (particularly rheumatoid arthritis and osteoarthritis). Non Surgical Treatment The good news is that the pain can often be relieved fairly easily with the right softer styled orthotic (even in those cases where there is concurrent plantar plate tears and capsulitis!), but its important to remeber that even if your no longer in pain, there is no magic cure to speeding up the healing process so one must take care of their feet for 6-12 weeks. As a rule of thumb a neuroma should always be treated conservatively where possible. This means icing and resting the area, trying to remove the causative factors, and providing postural control and support via metatarsal domes or, if needed, specialised pre-made or custom made orthotics.  Surgical Treatment Recently, an increasing number of procedures are being performed at specialist centers under radiological or ultrasound guidance. Recent studies have shown excellent results for the treatment of Morton's neuroma with ultrasound guided steroid injections, ultrasound guided sclerosing alcohol injections, ultrasound guided radiofrequency ablation and ultrasound guided cryo-ablation.  Overview OverviewHammertoes is a condition which causes one or more of the smaller toes to become bent upwards. The toe can be straightened but if ignored may become a permanent deformity. Each of the 4 smaller toes consist of 3 bones called phalanges, forming two interphalangeal joints. The toe bends at the proximal or first interphalangeal joint. Initially it can be straightened, but if left untreated, this can become a permanent deformity. Causes Hammer toes can be due to a number of things. Several factors are known to increase the risk of developing hammer toes. Some people are just structurally prone to develop hammer toes (hereditary) tight footwear is an important factor in the cause of hammer toes as well as providing the pressure that causes the symptoms, weaker small muscles in the foot may also play a role.  Symptoms Pain upon pressure at the top of the bent toe from footwear. The formation of corns on the top of the joint. Redness and swelling at the joint contracture. Restricted or painful motion of the toe joint. Pain in the ball of the foot at the base of the affected toe. Diagnosis Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe. If the deformed toe is very painful, your doctor may recommend that you have a fluid sample withdrawn from the joint with a needle so the fluid can be checked for signs of infection or gout (arthritis from crystal deposits). Non Surgical Treatment If you have hammer toe, avoiding tight shoes and high heels may provide relief. Initial (non-surgical) treatment for hammer toe involves wearing shoes with plenty of room in the toe area. Shoes should be at least one-half inch longer than the longest toe. Stretching and strengthening exercises for the toes (such as picking up items with the toes or stretching the toes by hand) are also recommended. Sometimes orthopedists recommend special pads, cushions, or slings to help relieve the pain of hammer toe. Surgical Treatment Surgery to correct for a hammertoe may be performed as an outpatient procedure at a hospital, surgery center, or in the office of your podiatrist. There are multiple procedures that can be used depending on your individual foot structure and whether the deformity is flexible or rigid. There may be a surgical cut in the bone to get rid of an exostosis, or a joint may be completely removed to allow the toe to lay straight.  Prevention Hammertoe can usually be prevented by wearing shoes that fit properly and give the toes plenty of room. Don?t wear shoes with pointed or narrow toes. Don?t wear shoes that are too tight or short. Don?t wear high-heeled shoes, which can force the toes forward. Choose shoes with wide or boxy toes. Choose shoes that are a half-inch longer than your longest toe. If shoes hurt, don?t wear them.
Overview
 A bunion is an unnatural, bony hump that forms at the base of the big toe where it attaches to the foot. Often, the big toe deviates toward the other toes. When this occurs, the base of the big toe pushes outward on the first metatarsal bone, which is the bone directly behind the big toe, forming a bunion. If this happens on the little toe and fifth metatarsal, it's called a bunionette. Because a bunion occurs at a joint, where the toe bends in normal walking, your entire body weight rests on the bunion at each step. Bunions can be extremely painful. They're also vulnerable to excess pressure and friction from shoes and can lead to the development of calluses. A bunion is an unnatural, bony hump that forms at the base of the big toe where it attaches to the foot. Often, the big toe deviates toward the other toes. When this occurs, the base of the big toe pushes outward on the first metatarsal bone, which is the bone directly behind the big toe, forming a bunion. If this happens on the little toe and fifth metatarsal, it's called a bunionette. Because a bunion occurs at a joint, where the toe bends in normal walking, your entire body weight rests on the bunion at each step. Bunions can be extremely painful. They're also vulnerable to excess pressure and friction from shoes and can lead to the development of calluses.Causes The most common cause of bunions is poor footwear. Poorly fitted shoes, high heeled shoes or shoes with a narrow toe area can all cause bunions or make bunions worse. Bunions can be hereditary and they can be associated with poor foot biomechanics such as overpronation or flat feet. Rheumatoid arthritis or some diseases of the nervous system can also cause bunions. Symptoms No matter what stage your bunion is in, you can be in pain. Though bunions take years to develop, you can experience pain at any stage. Some people don?t have bunion pain at all. Pain from a bunion can be severe enough to keep you from walking comfortably in normal shoes. The skin and deeper tissue around the bunion also may become swollen or inflamed. Diagnosis A simple visual exam is all it will take for your doctor to determine whether you have a bunion. He or she may also ask you to move your big toe in order to ascertain your range of motion. Your doctor may also look for any inflammation, redness, or pain. X-rays can help your doctor determine the severity and cause of the bunion. Your doctor may also ask you questions about your footwear, the symptoms you are experiencing, and if other family members also suffer from the condition. All these factors will help him or her diagnose you properly. Non Surgical Treatment Bunions may be treated with proper shoes and corrective inserts such as toe spacers, bunion or toe separators, as well as bunion cushions and splints. In extreme cases, surgery may be needed to remove the bony enlargement of the first metatarsal bone, realigning the bone, or straightening the big toe.  Surgical Treatment If the above simple measures do not make you comfortable, an operation may improve the situation. An operation will not give you an entirely normal foot, but it will correct the deformity of the big toe and narrow your foot back towards a more desirable shape. There are a lot of different operations for bunions, depending on the severity of the deformity, the shape of your foot and whether arthritis has developed in the big toe joint. An orthopaedic surgeon who specialises in foot & ankle surgery can advise you on the best operation for your foot. However, an operation may not make your foot narrow enough to wear tight shoes, nor can it fully restore the strength of the big toe. Prevention Bunions often become painful if they are allowed to progress. But not all bunions progress. Many bunion problems can be managed without surgery. In general, bunions that are not painful do not need surgical correction. For this reason, orthopaedic surgeons do not recommend ?preventive? surgery for bunions that do not hurt, with proper preventive care, they may never become a problem. Overview
Feet are supposed to roll inward as a part of every step you take. This helps them to mold to the various terrain that they step on (sand, rocks, various obstacles) without injury. This is called pronation. But, when your feet roll inward excessively, problems often arise. Excessive inward rolling of the feet and ankles is called over-pronation. Sometimes, people who over-pronate are told they have ?flat feet?. The term ?flat feet? can be misleading. When standing, body weight causes the arch of most feet to flatten out somewhat. This does not mean they become flat like pancakes (though some feet do). Instead, the arch shape gets longer and flatter and the arch height gets lower.  Causes Excess stress on the inner surface of the foot can cause injury and pain in the foot and ankle. Repeated rotational forces through the shin, knee, thigh and pelvis also place additional strain on the muscles, tendons and ligaments of the lower leg. Symptoms Symptoms can manifest in many different ways. The associated conditions depend on the individual lifestyle of each patient. Here is a list of some of the conditions associated with over Pronation. Hallux Abducto Valgus (bunions). Hallux Rigidus (stiff 1st toe). Arch Pain. Heel Pain (plantar Facsitus). Metatarsalgia (ball of the foot pain). Ankle Sprains. Shin Splints. Achilles Tendonitis. Osteochondrosis. Knee Pain. Corns & Calluses. Flat Feet. Hammer Toes. Diagnosis One of the easiest ways to determine if you overpronate is to look at the bottom of your shoes. Overpronation causes disproportionate wear on the inner side of the shoe. Another way to tell if you might overpronate is to have someone look at the back of your legs and feet, while you are standing. The Achilles tendon runs from the calf muscle to the heel bone, and is visible at the back of the ankle. Normally it runs in a straight line down to the heel. An indication of overpronation is if the tendon is angled to the outside of the foot, and the bone on the inner ankle appears to be more prominent than the outer anklebone. There might also be a bulge visible on the inside of the foot when standing normally. A third home diagnostic test is called the ?wet test?. Wet your foot and stand on a surface that will show an imprint, such as construction paper, or a sidewalk. You overpronate if the imprint shows a complete impression of your foot (as opposed to there being a space where your arch did not touch the ground).  Non Surgical Treatment The way a foot orthotic works is by altering the weight-bearing surface of the foot. The simulated foot improvement is only possible when standing still with full weight applied. Orthotics are of little help through most of the actual walking cycle. observationPatients may experience some symptom relief, but the orthotic cannot correct the internal osseous misalignment. Over-the-counter foot orthotics are usually of little help and wear out quickly. Custom-made foot orthotics, obtained through your doctor's office, are generally expensive. Though they last longer and have less chance of ill-effects than OTC brands, they still need to be replaced often. Over a lifetime, an individual can spend several thousands of dollars in total costs associated with orthotics and see little or no results. This is because orthotics only work when you are wearing them and do not treat the cause of the problem. In many cases, the external pressure points created by orthotics can cause more problems than solutions. Blisters, sore feet, sore joints and many other long-term complications can arise as a consequence of wearing orthotics. Prevention Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push: Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board. Overview
Sever?s disease is a common cause of heel pain in children especially in the young and physically active. Severs disease is a painful bone disorder that results from inflammation (swelling) of the growth plate in the heel. A growth plate, also called an epiphyseal plate, is an area at the end of a developing bone where cartilage cells change over time into bone cells. As this occurs, the growth plates expand and unite. It is very important that damage to the growth plate is avoided. Causes The heel bone grows faster than the ligaments in the leg. As a result, muscles and tendons can become very tight and overstretched in children who are going through growth spurts. The heel is especially susceptible to injury since the foot is one of the first parts of the body to grow to full size and the heel area is not very flexible. Sever?s disease occurs as a result of repetitive stress on the Achilles tendon. Over time, this constant pressure on the already tight heel cord can damage the growth plate, causing pain and inflammation. Such stress and pressure can result from sports that involve running and jumping on hard surfaces (track, basketball and gymnastics). Standing too long, which puts constant pressure on the heel. Poor-fitting shoes that don?t provide enough support or padding for the feet. Overuse or exercising too much can also cause Sever?s disease. Symptoms Symptoms include complaints of pain or tenderness in the heel (or heels), discomfort when heel is squeezed, limping, and more severe pain after walking, running or playing sports. Sever?s disease is directly related to overuse of the bone and tendons in the heel. This can come from playing sports or anything that involves lots of heel movements and hard shoes such as cleats. It can be associated with starting a new sport, or the start of a new season. It occurs more commonly in children who pronate (feet roll inward), and involves both heels in more than half of patients. Diagnosis Your podiatrist will take a comprehensive medical history and perform a physical examination including a gait analysis. The assessment will include foot posture assessment, joint flexibility (or range of motion), biomechanical assessment of the foot, ankle and leg, foot and leg muscle strength testing, footwear assessment, school shoes and athletic footwear, gait analysis, to look for abnormalities in the way the feet move during gait, Pain provocation tests eg calcaneal squeeze test. X-rays are not usually required to diagnose Sever?s disease. Non Surgical Treatment It is important that those with Sever?s Disease are treated by a medical professional to reduce pain and allow children to continue to participate in sporting activities. The Athlete?s Foot recommends a visit to your local medical professional to be diagnosed correctly and receive specialised care. Symptoms include pain through the back of the heel where the Achilles tendon inserts into the heel bone, pain during activity especially running and jumping and the back of the heel may be tender to touch. Surgical Treatment The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Overview
 Achilles tendon rupture is an injury that affects the back of your lower leg. It most commonly occurs in people playing recreational sports. The Achilles tendon is a strong fibrous cord that connects the muscles in the back of your calf to your heel bone. If you overstretch your Achilles tendon, it can tear (rupture) completely or just partially. If your Achilles tendon ruptures, you might feel a pop or snap, followed by an immediate sharp pain in the back of your ankle and lower leg that is likely to affect your ability to walk properly. Surgery is often the best option to repair an Achilles tendon rupture. For many people, however, nonsurgical treatment works just as well. Achilles tendon rupture is an injury that affects the back of your lower leg. It most commonly occurs in people playing recreational sports. The Achilles tendon is a strong fibrous cord that connects the muscles in the back of your calf to your heel bone. If you overstretch your Achilles tendon, it can tear (rupture) completely or just partially. If your Achilles tendon ruptures, you might feel a pop or snap, followed by an immediate sharp pain in the back of your ankle and lower leg that is likely to affect your ability to walk properly. Surgery is often the best option to repair an Achilles tendon rupture. For many people, however, nonsurgical treatment works just as well.Causes People who commonly fall victim to Achilles rupture or tear include recreational athletes, people of old age, individuals with previous Achilles tendon tears or ruptures, previous tendon injections or quinolone use, extreme changes in training intensity or activity level, and participation in a new activity. Most cases of Achilles tendon rupture are traumatic sports injuries. The average age of patients is 29-40 years with a male-to-female ratio of nearly 20:1. Fluoroquinolone antibiotics, such as ciprofloxacin, and glucocorticoids have been linked with an increased risk of Achilles tendon rupture. Direct steroid injections into the tendon have also been linked to rupture. Quinolone has been associated with Achilles tendinitis and Achilles tendon ruptures for some time. Quinolones are antibacterial agents that act at the level of DNA by inhibiting DNA Gyrase. DNA Gyrase is an enzyme used to unwind double stranded DNA which is essential to DNA Replication. Quinolone is specialized in the fact that it can attack bacterial DNA and prevent them from replicating by this process, and are frequently prescribed to the elderly. Approximately 2% to 6% of all elderly people over the age of 60 who have had Achilles ruptures can be attributed to the use of quinolones. Symptoms The most common initial symptom of Achilles tendon rupture is a sudden snap at the back of the heels with intense pain. Immediately after the rupture, the majority of individuals will have difficult walking. Some individuals may have had previous complains of calf or heel pain, suggesting prior tendon inflammation or irritation. Immediately after an Achilles tendon rupture, most individuals will develop a limp. In addition, when the ankle is moved, the patient will complain of pain. In all cases, the affected ankle will have no strength. Once the Achilles tendon is ruptured, the individual will not be able to run, climb up the stairs, or stand on his toes. The ruptured Achilles tendon prevents the power from the calf muscles to move the heel. Whenever the diagnosis is missed, the recovery is often prolonged. Bruising and swelling around the calf and ankle occur. Achilles tendon rupture is frequent in elderly individuals who have a sedentary lifestyle and suddenly become active. In these individuals, the tendon is not strong and the muscles are deconditioned, making recovery more difficult. Achilles tendon rupture has been reported after injection of corticosteroids around the heel bone or attachment of the tendon. The fluoroquinolone class of antibiotics (such as ciprofloxacin [Cipro]) is also known to cause Achilles tendon weakness and rupture, especially in young children. Some individuals have had a prior tendon rupture that was managed conservatively. In such cases, recurrence of rupture is very high. Diagnosis During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if a complete rupture has occurred. Achilles tendon rupture can be diagnosed reliably with clinical examination, but if there?s a question about the extent of your Achilles tendon injury then your doctor may order a magnetic resonance imaging (MRI) scan. Non Surgical Treatment Treatment for a ruptured Achilles tendon often depends on your age, activity level and the severity of your injury. In general, younger and more active people often choose surgery to repair a completely ruptured Achilles tendon, while older people are more likely to opt for nonsurgical treatment. Recent studies, however, have shown fairly equal effectiveness of both operative and nonoperative management. Nonsurgical treatment. This approach typically involves wearing a cast or walking boot with wedges to elevate your heel, which allows your torn tendon to heal. This method avoids the risks associated with surgery, such as infection. However, the likelihood of re-rupture may be higher with a nonsurgical approach, and recovery can take longer. If re-rupture occurs, surgical repair may be more difficult.  Surgical Treatment There are two types of surgery to repair a ruptured Achilles tendon. In open surgery, the surgeon makes a single large incision in the back of the leg. In percutaneous surgery, the surgeon makes several small incisions rather than one large incision. In both types of surgery, the surgeon sews the tendon back together through the incision(s). Surgery may be delayed for about a week after the rupture, to let the swelling go down. Overview
The field of leg length inequalities or leg length discrepancy often abbreviated as LLD is well documented and understood. There are two types of short legs; functional (functional LLD) and structural (true LLD). A functional short leg occurs as a result of muscle imbalances, pelvic torsion or other mechanical reasons. The millimeters of ?appearing? short are typically less than 10, and are do not appear on Xray. This article is about structural or anatomical short legs.  Causes The causes of LLD may be divided into those that shorten a limb versus those that lengthen a limb, or they may be classified as affecting the length versus the rate of growth in a limb. For example, a fracture that heals poorly may shorten a leg slightly, but does not affect its growth rate. Radiation, on the other hand, can affect a leg's long-term ability to expand, but does not acutely affect its length. Causes that shorten the leg are more common than those that lengthen it and include congenital growth deficiencies (seen in hemiatrophy and skeletal dysplasias ), infections that infiltrate the epiphysis (e.g. osteomyelitis ), tumors, fractures that occur through the growth plate or have overriding ends, Legg-Calve-Perthes disease, slipped capital femoral epiphysis (SCFE), and radiation. Lengthening can result from unique conditions, such as hemihypertrophy , in which one or more structures on one side of the body become larger than the other side, vascular malformations or tumors (such as hemangioma ), which cause blood flow on one side to exceed that of the other, Wilm's tumor (of the kidney), septic arthritis, healed fractures, or orthopaedic surgery. Leg length discrepancy may arise from a problem in almost any portion of the femur or tibia. For example, fractures can occur at virtually all levels of the two bones. Fractures or other problems of the fibula do not lead to LLD, as long as the more central, weight-bearing tibia is unaffected. Because many cases of LLD are due to decreased rate of growth, the femoral or tibial epiphyses are commonly affected regions. Symptoms Often there are few or no symptoms prior to the age of 25-35. The most common symptom is chronic lower back pain, but also is frequently middle and upper back pain. Same-sided and repeated injury or pain to the hip, knee and/or ankle is also a hallmark of a long-standing untreated LLD. It is not uncommon to have buttock or radiating hip pain that is non-dermatomal (not from a disc) and tends to go away when lying down. Diagnosis The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used. Non Surgical Treatment Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).  Surgical Treatment The bone is lengthened by surgically applying an external fixation device to the leg. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins, or both. A small crack is made in the bone and the frame creates tension when the patient or family member turns its dial. This is done several times each day. The lengthening process begins approximately five to 10 days after surgery. The bone may lengthen 1 millimeter per day, or approximately 1 inch per month. Lengthening may be slower in a bone that was previously injured. It may also be slower if the leg was operated on before. Bones in patients with potential blood vessel abnormalities, such as cigarette smokers, may also need to be lengthened more slowly. The external fixator is worn until the bone is strong enough to support the patient safely. This usually takes about three months for each inch. Factors such as age, health, smoking and participation in rehabilitation can affect the amount of time needed. |
